The Postpartum Core Canister
The Postpartum Core Canister: Why Your Breathing Strategy is the Secret to Fixing Leaking, Pain, and Diastasis Recti
If you’ve been trying to heal your postpartum body by slamming your core with endless crunches, planks, or isolated Kegels, I need you to hit the pause button.
True postpartum core and pelvic floor recovery doesn't START with how hard you can squeeze a muscle. It starts with pressure management and breathing mechanics.
As a pelvic floor physical therapist, birth doula, and mom of two, I see so many women struggle with lingering symptoms like leaking, pelvic pain, pain with intercourse, and diastasis recti (abdominal separation). They think their muscles are just weak. But the truth? Their core canister is not functioning optimally and their pressure management system is completely disrupted.
Let’s look at the actual clinical science of how your deep core is designed to move, and how a common "pregnancy posture shift" might be sabotaging your recovery.
What is the Core Canister?
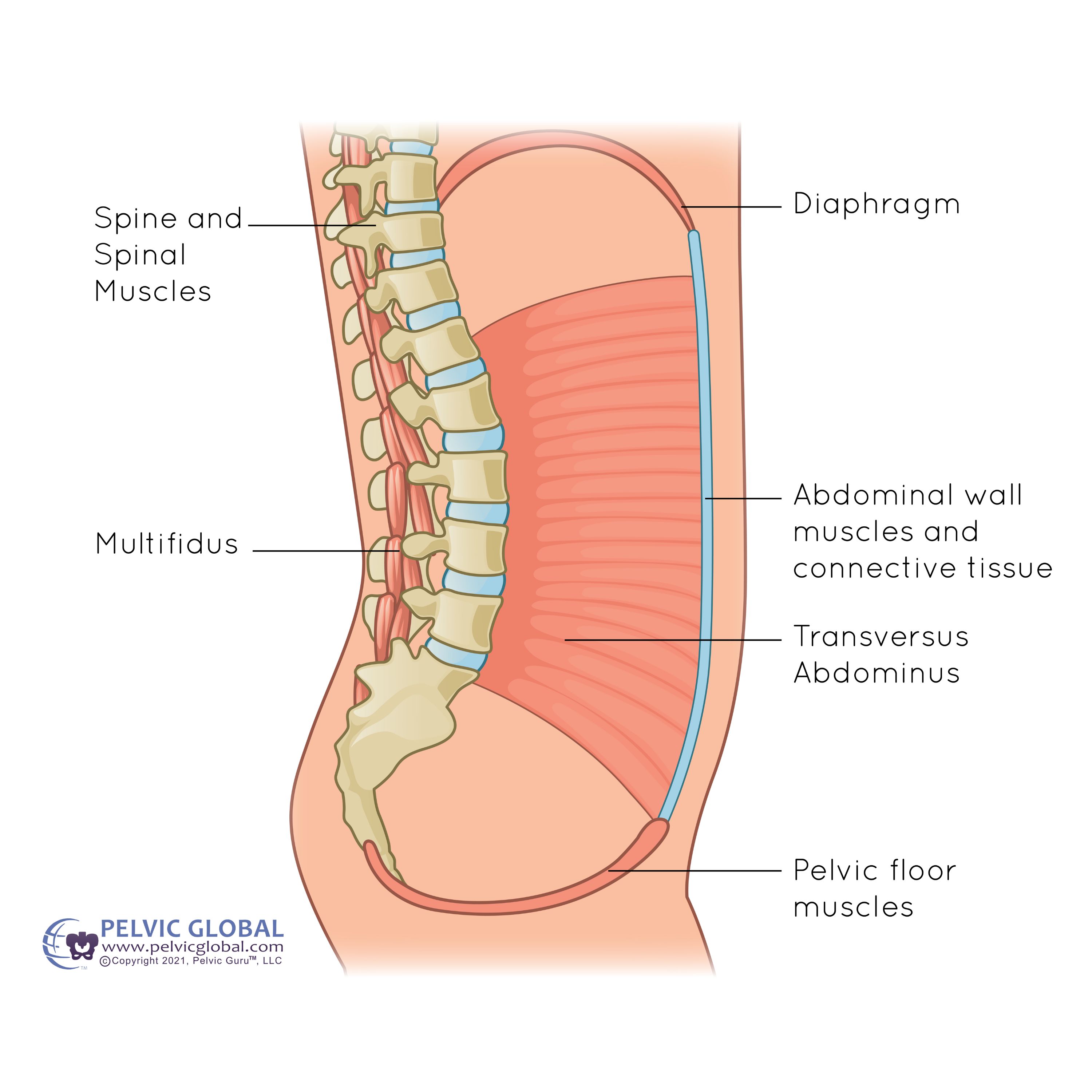
Think of your deep core not as a single flat sheet of abdominal muscle, but as a dynamic, pressurized cylinder or canister. This canister is made up of four essential walls that must work in absolute harmony:
The Top: Your diaphragm, a dome-shaped muscle that sits beneath your lungs and acts as the primary driver for pulling air into your body.
The Bottom: Your pelvic floor, a group of muscles that supports your pelvic organs, anchors to the base of your spine and pelvis to act as a vital structural stabilizer, and keeps you continent.
The Front & Sides: Your abdominal muscles (specifically the deep transversus abdominis), which wrap all the way around from the back to the front like a built-in corset.
The Back: Your multifidi, the deep, small muscles along your spine that dictate spinal stability.
For this canister to protect your spine, support your organs, and keep you from leaking when you move, all four walls have to communicate. If even one wall is out of sync, the pressure inside the canister becomes unmanaged.
Shallow vs. Deep: Are You Breathing Like a Stressed-Out Mom?
To get the canister working again, we have to look at your breathing mechanics. Try this quick assessment right now: place one hand on your chest and take a deep breath in. What do you notice? Does your chest rise straight up toward your chin?
If you see or feel a significant chest lift, you are trapped in a shallow breathing pattern.
When you breathe into your upper chest, air only fills the very top of your lungs. This severely limits the movement and mobility of your rib joints and stops your diaphragm from doing its job.
In an optimal system, when you inhale, your diaphragm should descend down and flatten, while your ribs expand out and up in a 360-degree direction (often called a bucket handle pattern). As the diaphragm moves down on the inhale, the pelvic floor gently moves down and lengthens to catch that internal pressure. On the exhale, the diaphragm moves back up, and the pelvic floor reflexively lifts and contracts.
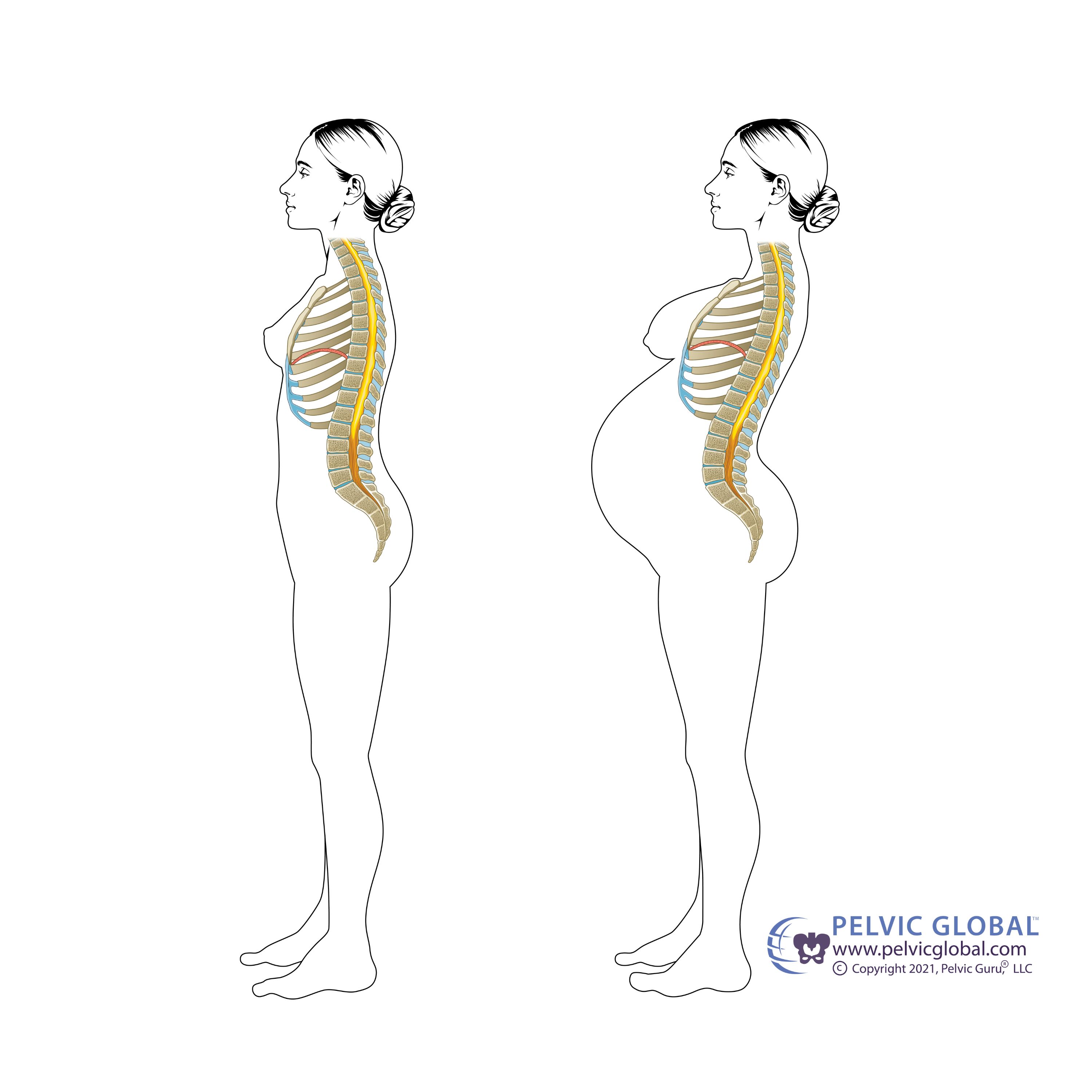
The Pregnancy Disruption: How Your Canister Fails
During pregnancy, this beautiful, reflexive system gets totally disrupted. As your baby grows, your internal organs are pushed upward, your rib cage flares out, and your pelvis tilts forward. Your body naturally stays stuck in this shifted posture postpartum.
When your posture is unstacked, your breathing mechanics fail. Because you can no longer drop your diaphragm cleanly, your core canister cannot manage internal pressure effectively.
The Pressure Trap: Leaking & Diastasis Recti
When you cough, sneeze, run, or lift a heavy car seat, your body generates intra-abdominal pressure. If your canister is misaligned, that force has nowhere to go. Instead of being absorbed by your entire core system, it shoots:
Down into the pelvic floor, resulting in leaking, pelvic heaviness, or pain with intercourse.
Out into the abdominal wall, pushing against your healing tissues and worsening diastasis recti.
Clinical research by Dr. Paul Hodges and Michelle Smith (2007) reveals that women dealing with stress urinary incontinence actually have increased hyper-reflexive tension in their pelvic floor and outer abdominal muscles. Their bodies are desperately over-gripping and bracing to find stability because their primary pressure management system—the breathing canister—is completely broken.
You don’t need to force more isolated contractions into an already exhausted system; you need to restore the canister's alignment.
How to Start Restoring Your System
True postpartum core and pelvic floor rehabilitation is about learning how to align your bones so your muscles can turn on automatically. Over the next few weeks, we are going to focus entirely on unpacking your pelvic mechanics, mastering pressure management, and building functional strength.
To help you visualize exactly how these mechanics work, I’ve broken down the anatomy and live breathing corrections in my latest video.
📺 Watch the full breakdown below to see the exact difference between a shallow breath and a functional canister breath:
Let's Build Your Restoration Plan
Motherhood is an athletic endurance sport. Stop training for it using generic fitness apps that ignore your pressure system and alignment.
If you’re tired of white-knuckling your way through postpartum symptoms and are ready to move pain-free, I am here to help you.
In-Home Concierge Care (Mercer County, NJ): I bring specialized, clinical Doctor of Physical Therapy evaluations and hands-on pelvic rehab straight to your living room.
Virtual Pelvic Health Consultations: No matter where you are located, we can hop on a screen together to troubleshoot your breathing patterns, assess your alignment, and build your custom postpartum roadmap.
Book your free 15 minute Consultation Call Today!!
Scientific References
Hodges, P. W., Sapsford, R., & Pengel, L. H. M. (2007). Postural and respiratory functions of the pelvic floor muscles. Neurourology and Urodynamics, 26(3), 362-371.
Smith, M. D., Coppieters, M. W., & Hodges, P. W. (2007). Postural response of the pelvic floor and abdominal muscles in women with and without incontinence. Neurourology and Urodynamics, 26(3), 377-385.
Sapsford, R. R., Hodges, P. W., Richardson, C. A., Cooper, D. H., Markwell, S. J., & Jull, G. A. (2001). Co-activation of the abdominal and pelvic floor muscles during voluntary exercises. Neurourology and Urodynamics, 20(1), 31-42.